In 2023, Egypt became the first country in the world to receive the World Health Organization’s “gold tier” recognition for progress toward eliminating hepatitis C. For decades, Egypt had one of the highest hepatitis C prevalence rates in the world, with roughly ten percent of the population infected and some rural communities reporting rates as high as twenty-four percent [1]. The virus was a national catastrophe, responsible for millions of chronic infections and a large proportion of liver disease mortality [1].
The country responded with an rigorous national program, characterized by a centralized treatment network, price negotiations for antiviral drugs, and a massive “test and treat” campaign which transformed the landscape of care [1]. In 2018 alone, Egypt screened nearly 57 million people for hepatitis C and ultimately treated more than four million patients [2]. Cure rates approached ninety-eight percent, and within a decade national prevalence fell from roughly ten percent to under half a percent [1]. Measured by the WHO’s elimination framework, the program was given a gold-tier designation, which requires that at least 80 percent of people living with hepatitis C be diagnosed and that at least 70 percent of those diagnosed receive treatment [3] [4]. Egypt surpassed both thresholds, diagnosing 87 percent of infected individuals and treating 93 percent of them [5].

The messaging of the distinction is simple and clear: this is what global health success looks like.
By all normative measures, Egypt’s resounding success story is the “gold standard.” I must acknowledge my own limited experience when I say this, but what then would the WHO call the work of ASHA workers in the bidis of Gungralchatra, Mysore, who strive to screen an entire taluk of women for HPV? What would they say about efforts of Community Health Workers and Promotoras in the Delta Region of Southeast Arkansas to bridge transportation barriers for preventative health?
What kinds of health problems are capable of becoming “gold standards” in the first place? Can we even set a standard to begin with?
Egypt’s achievement represents what public health dreams of: a national program that mobilizes political will, deploys effective treatment, and measurably reduces disease. Yet the very features that allow us to denote the program as a success also reveal something about the epistemology of global health. Hepatitis C elimination fits neatly into the architecture of modern public health metrics. The disease is identifiable through a clear diagnostic test. Treatment is curative. Outcomes are measurable and occur within relatively short time frames. Incidence, mortality, and prevalence can all be quantified and tracked against global benchmarks. This is exactly the kind of problem that global health knows how to solve. But it is not the only kind of health crisis that exists.
Health and the human condition exist as a diaspora– chronic disease, environmental exposures, disability, mental illness, and structural health inequalities– that rarely conforms to a static model. They may unfold slowly, unevenly, or invisibly across populations. Their effects may be shaped by housing, labor, poverty, violence, and political neglect. These quandaries are difficult to stuff into the clean epidemiological boxes that monolithic global health institutions rely upon.
Global health tends to see most clearly the problems that can be counted.
I’m reminded of a metaphor Jamaica Kincaid shares in her amazing work A Small Place. On tourism in Antigua, she writes:
The resort is not by design falsifying reality. It’s an experience designed so visitors never have to see or think about where the sewage goes. In my Science Olympiad days (groan) I spent time pouring over the CDC’s field epidemiology handbook. I see terms pop up from this in most every discussion of global public and community health. Incidence rates, stratification, aggregation, HALYs/DALYs. This was a topic discussed at length in an amazing course I am taking this semester, ANTH 389: Empire & Medicine. In a landscape littered with INGOs and NGOs, industrial giants, private capital, humanitarian organizations, and nation-states, global health has been to an extent been built on neoliberal principles. The very fabric of global health is in large part predicated on quantifiable metrics that can make for persuasive, legible, and fundable health models and systems. Like the resort, the system is designed to highlight certain realities that more comfortably fit a mold. What does that leave out, though?
Consider Pakistan, which today carries one of the largest hepatitis C burdens in the world, with an estimated eight to ten million people living with the virus. [6] The scientific tools that enabled Egypt’s success (accurate diagnostics and curative antiviral treatments) are available there as well. However, Its healthcare system is decentralized across provinces, screening capacity is uneven, and ongoing transmission persists through unsafe medical injection practices [6] [7]. In this context, the idea of screening tens of millions of people through a coordinated national campaign is categorically unrealistic.
The result is a strange paradox. Pakistan faces a hepatitis C burden comparable to Egypt’s historic epidemic, yet it is unlikely to receive “gold tier” recognition anytime soon. Not because the disease is less urgent, or the clinicians less committed, but because the conditions required to meet the benchmark are themselves sparsely represented across the globe. Egypt’s hepatitis C program deserves recognition, and provides us landmark learnings. But, we should seek to incorporate the learnings into crafting an epistemological shift that prevents us from obscuring systems, practices, or bodies that are difficult to “count”.
I feel the key to this shift lies in the grassroots. I am immediately reminded of the invaluable work of community health workers in many parts of the world. In India for example, ASHA (Accredited Social Health Activists) are uniquely positioned in intersectional roles that involve trust building, health education, and the esoteric knowledge of complex social dynamics [8]. These efforts may reduce risk over years rather than months, but prevent illness rather than cure it, and strengthen local health infrastructures in ways that are difficult to translate into clean epidemiological indicators. The work is critical to maintaining health, and critical to unify into global health perspectives.
The shift will take forgetting everything we think we know, starting anew, and asking “What if?”
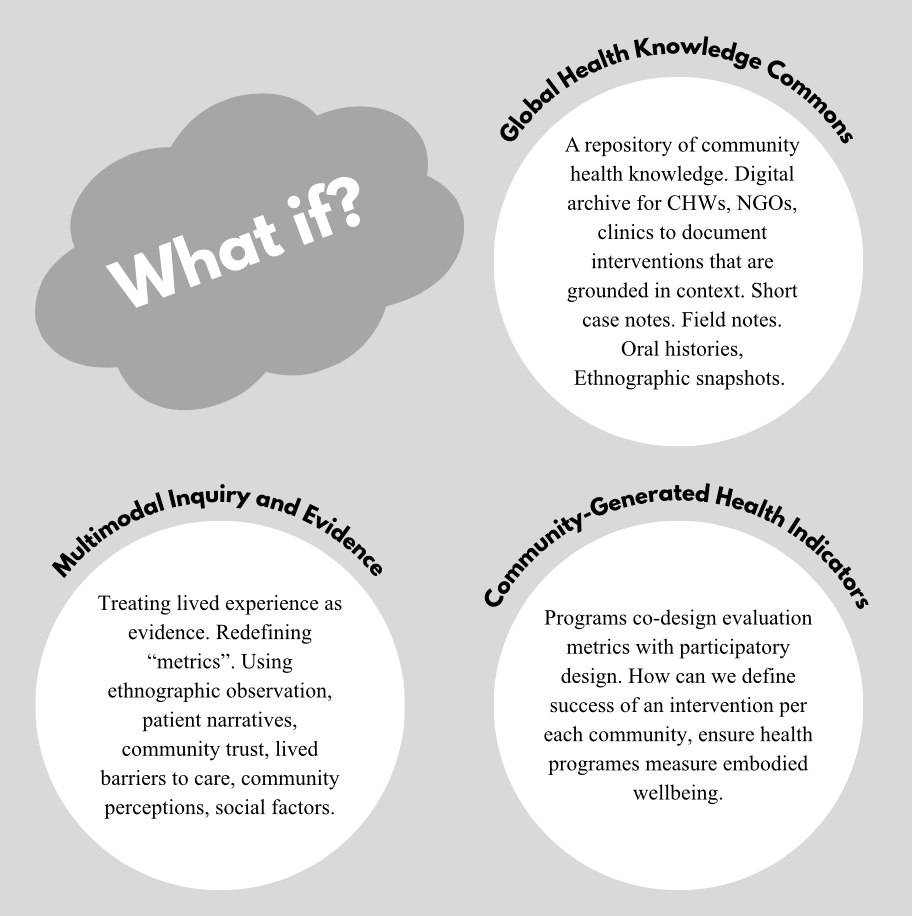
See my Global Health Commons Lakehouse Prototype: https://sasaigoli05.github.io/ghcommons_prototype
REFERENCES
- Gomaa, A., Allam, N., Elsharkawy, A., El Kassas, M., & Waked, I. (2021). Egypt’s ambitious strategy to eliminate hepatitis C virus: A case study. Global Health: Science and Practice, 9(2), 187–200. https://pmc.ncbi.nlm.nih.gov/articles/PMC8087425/
- Esmat, G., Metwally, A., El Kassas, M., Abdel-Razek, W., El Akel, W., Gomaa, A., & Waked, I. (2020). Emerging from the screening of 57 million citizens and treating 4 million patients: Future strategies to eliminate hepatitis C from Egypt. Expert Review of Anti-infective Therapy, 18(12), 1105–1114. https://pubmed.ncbi.nlm.nih.gov/32302245/
- World Health Organization. (2023, October 9). WHO commends Egypt for its progress on the path to eliminate hepatitis C. https://www.who.int/news/item/09-10-2023-who-commends-egypt-for-its-progress-on-the-path-to-eliminate-hepatitis-c
- Africa Centres for Disease Control and Prevention. (2023). The Arab Republic of Egypt achieves historic gold tier certification in hepatitis C elimination. https://africacdc.org/news-item/the-arab-republic-of-egypt-achieves-historic-gold-tier-certification-in-hepatitis-c-elimination/
- World Health Organization Regional Office for the Eastern Mediterranean. (2023). Egypt becomes the first country to achieve WHO validation on the path to elimination of hepatitis C. https://www.emro.who.int/media/news/egypt-becomes-the-first-country-to-achieve-who-validation-on-the-path-to-elimination-of-hepatitis-c.html
- Luby, S. P., Qamruddin, K., Shah, A. A., Omair, A., Pahsa, O., Khan, A. J., Rasheed, S., Fisher-Hoch, S., & McCormick, J. B. (1997). The relationship between therapeutic injections and high prevalence of hepatitis C infection in Hafizabad, Pakistan. Epidemiology and Infection, 119(3), 349–356. https://pmc.ncbi.nlm.nih.gov/articles/PMC12728702/
- Abbas, F., Riaz, S., Ahmad, Z., Ullah, S., Haq, I., Ahmad, A., & Khan, M. (2024). Pakistan’s progress towards hepatitis C elimination: Achievements and remaining challenges. Journal of Viral Hepatitis, 31(1), e145–e156. https://pmc.ncbi.nlm.nih.gov/articles/PMC11129505/
- Chawla, S., Kumar, C., Bose, M., & Shrivastav, S. M. (2025). Performance and challenges of Accredited Social Health Activists (ASHAs) in delivering key Maternal and Newborn Health (MNH) services in India: A systematic review and meta-analyses. SSM – Health Systems, 5, 100134. https://doi.org/10.1016/j.ssmhs.2025.100134
Leave a Reply